How Physician Resilience Training Changed a Georgia Doctor’s Life and Career
Dr. Michael Lipscomb , ApolloMD Chief Quality and Patient Safety Officer, has practiced emergency medicine for almost 25 years and possesses extensive experience in optimizing both department flow and patient satisfaction.
, ApolloMD Chief Quality and Patient Safety Officer, has practiced emergency medicine for almost 25 years and possesses extensive experience in optimizing both department flow and patient satisfaction.
After noticing the impact of stress on his career, Dr. Lipscomb developed a renewed focus on cultivating personal and professional wellness among health care professionals. He recently spoke on the topic at the Ohio Hospital Association Annual Meeting. Highlights from the presentation are noted here.
_________________________________________________________
Resilience is a topic that has been gaining attention but is perhaps still not well-comprehended. It is my goal to help you understand, through the lens of a physician – specifically me – how non-resilience and non-wellness affects us as a profession and, as a result, affects our patients. I will also share how I have helped – but not fixed – my problem.
Some of what I talk about pertains to emergency physicians, but it applies to anyone in health care.
As Chief Quality Officer for ApolloMD, I work to optimize quality in multiple emergency medicine, hospital medicine, anesthesiology, and radiology practices. These are physicians and advanced practice clinicians who are already overburdened with paperwork and other non-patient-facing tasks. I routinely see issues related to wellness and resilience, but as a physician, I may be one of the worst authorities on these subjects. Our training teaches us not to be mindful and not to take care of ourselves. So this is where I’m going in a discussion of wellness – or unwellness – of physicians and APCs.
‘A LITTLE UNWELL’ IS A EUPHEMISM: PHYSICIAN BURNOUT IS SERIOUS
Let’s start with the scope of the problem.
Physicians have the highest suicide rates of any profession – about one physician each day – which is a higher ratio than even military personnel. If we think of wellness as a bell curve, with the lowest part of the bell curve representing those who commit suicide, we see indicators that the entire medical professional curve has shifted.
Physician burnout (especially emergency physician burnout) is common and can be defined as emotional or physical exhaustion brought on by mental stress or lack of enthusiasm at work. We physicians, as a group, are emotionally and physically exhausted by stress and lack of enthusiasm for what we do. More regulations, more time on the computer away from patients, more scrutinized by metrics – all of this has beaten us down.
Stress is a necessary part of our job as physicians, but that alone does not necessarily lead to burnout. Burnout occurs when the stress becomes prolonged and uncontrolled, and when we don’t have the time or tools necessary for recovery. So, why do we have this problem in medicine? A few reasons:
- We are highly successful, type-A personalities who are scared to fail. Most of us were at the top of our class and continue to work at that level.
- Patients come first; we come last. In medical school, we’re taught that patient care trumps anything else, even your own health and wellness. When the phone rings or beeper buzzes, you drop everything and go!
- Backward, as well as forward-thinking habits, remove us from the present moment. We’re wondering about patients from yesterday and thinking about our busy schedule tomorrow. The constant switching around derails us from our ability to concentrate on the tech, the nurse, or even the patient who is in front of us right now.
MY PROBLEM
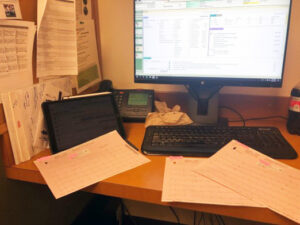
I spend the majority of my time behind my computer. This is my world. This picture is not staged. This was an “OMG moment” where I stepped back and took a picture of exactly what was going on at the time I made a significant medical error.
There’s a lot of noise here. In addition to the EHR, there’s an iPad full of texts and emails I need to answer. I have EKGs getting dropped over my shoulder. I have my to-do list tucked behind my iPad and the phone could go off at any moment or there may be an overhead page for me.
What happened here? In the middle of all this noise, a child with appendicitis received a CT scan that he didn’t need. The error was ultimately my fault, I’m the one who ordered the test. However, it turned out he didn’t need the scan. I was able to get a surgical consult and when we agreed that everything pointed to appendicitis, we sent the child right down to the pediatric hospital. I filled out paperwork, spoke to the nurse, talked to the patient’s mom, contacted the pediatric surgeon, and arranged everything. I happily moved on to my next patient.
But, I forgot to cancel the CT order. Long after I thought this child had left, I got a call from radiology with results confirming appendicitis and I realized this patient received unnecessary X-rays.
Outside of this event, we actually had a really busy day with 114 patients and only one patient that left without being seen, numbers which are quite good. However, I didn’t reflect on the number of patients treated. I remembered only the negative, including my mistake with the young patient. I knew that I may go to peer review for the incident or get a patient complaint about the CT scan. We’re wired to remember the negative and many of our policies reinforce the negative not positive; in other words, the hospital can be a breeding ground for emergency physician burnout.
RECOLLECTION: THE BEGINNINGS OF PHYSICIAN RESILIENCE TRAINING
I spent a few minutes collecting myself. On that day, it was a child with appendicitis, but it could just as easily have been a child who drowned or a severe head injury from a car accident. Or maybe, one of the toughest for me, the death of an elderly patient whose spouse said, “Doc, I just lost my best friend of 65 years.”
As medical personnel, our environment can lead us to uncontrolled stress.
Day in and day out, this can lead to burnout, depression, and other problems. Let’s look at two specific communication examples that can make the situation worse:
Reflexive Thinking
When we’re not in the present, we frequently fall into a reflexive mode of actions and answers. Our brain is hardwired based upon past experiences and we automatically respond from the amygdala. This is the reptilian part of the brain that can make us jump from fear and also make us respond to our colleagues without even thinking about what we are saying.
Filters
Sometimes it’s just the viewpoint we have of the world that hinders our ability to connect with others. Taking a pause to understand will at least give us a chance at an optimal outcome for that patient and the ability to re-direct conversations that aren’t going so well.
PHYSICIAN, HEAL THYSELF: HOW TO COMBAT PHYSICIAN BURNOUT FROM THE HOSPITAL’S POINT OF VIEW
What are the components of wellness? In 2017, the New England Journal of Medicine published a study identifying three parts of well-being in a hospital or any organization. The first two (Culture of Wellness & Efficiency of Practice) are things that can be controlled by the hospital. The third (Personal Resilience) is a responsibility of the individual:
Culture of Wellness
The attitudes and behaviors of an organization determine much of the culture for its people. What are the undertones of your emails? Are you interested in the well-being of individuals? Are you celebrating the wins, the great work, and optimal patient care?
Efficiency of Practice
How does the organization support both the clinical work and the energy spent to get it done? Are you helping with case management? Are you providing adequate resources to help staff meet hospital goals?
Personal Resilience
These individual skills, values, and behaviors lead to habits that impact wellness. These are more challenging to measure, as physicians and APCs seem disinclined to help themselves. Organizations can assist in the development of skills by facilitating physician resilience training and workshops.
MY SOLUTION
In 2018, I was fortunate enough to hear a physician talk about a path that helped him. He described burnout, saying that while he couldn’t put a finger on it, something seemed wrong with his life. So, he went to a three-day workshop and suggested I consider one, too. I went through three days of training in a program that, much like diet and exercise, requires ongoing work. Some of the sample exercises:
- Being present and in the moment – We went outside around a lake and were told to focus for 10 minutes on nothing but the beautiful scenery. We all failed, admitting that after a few minutes our minds wandered to other tasks, but at least the practice was now introduced.
- Phone a friend — We were assigned to call a friend or colleague and ask how we functioned when on our “D-game” state. I called our medical director and after a few minutes, he told me a story about an interaction I’d had with a nurse in which I had been so distracted that I inadvertently belittled her. I sought her out to apologize soon after completing the workshop.
At our company’s annual leadership conference, I speak frequently about quality. Two years ago, rather than speak for an hour about MIPS and other quality measures, I spent about 10-15 minutes on the obligatory stuff and then spent the balance of my time talking about how cultivating wellness and resilience has helped me as one of the best solutions to physician burnout.
From a quality standpoint, wellness is the single most important attribute to instill in our teams.
Now, two years later, we have a commitment to understanding that our success as physicians and as a company starts with employee wellness. Our new vision statement reflects that with a mandate of “Healthy Clinicians. Healthy Patients. Healthy Communities.” We’re getting traction. We have a wellness committee; we started cohorts of physicians and APCs to learn the wellness basic concepts, and we’re talking to physicians who struggle. We all need a champion.
For more information about the ApolloMD Quality Team or to speak with Dr. Lipscomb directly, you may email him at mlipscomb@apollomd.com.
_______________________________________________________________
Dr. Mike Lipscomb began practicing Emergency Medicine in 1997 as a Clinical Instructor for the University of Michigan. In 2000, he joined ApolloMD at Wellstar North Fulton Hospital, becoming Medical Director of the department in 2005. Dr. Lipscomb has served on multiple committees at the hospital, most recently completing terms of Secretary, Treasurer, and Chief of Staff, and he continues to serve on the Medical Executive Committee. In 2013, ApolloMD was excited to welcome Dr. Lipscomb to the corporate team to oversee clinical operations of hospitals in the Southeast. With extensive experience in optimizing emergency department flow, EMR use, and patient satisfaction, Dr. Lipscomb became Chief Quality Officer for ApolloMD in 2016. Dr. Lipscomb received his medical degree from The University of Texas Southwestern Medical Center at Dallas and completed residency training in Emergency Medicine at The University of Michigan Medical School.
Please correct the following fields before submitting:
- Field Name is required
- Field Email is required